NHS activity and performance summary: May and June 2021
Report summarising data on activity and performance in the Welsh NHS for May and June 2021.
In this page
This statistical release provides a summary of NHS Wales activity and performance data.
New data relating to calls to the ambulance service, emergency department attendances and admissions to hospital from major emergency departments are provided for the month of April 2021.
New data relating to referrals for first outpatient appointments, diagnostic and therapy waiting times (DATS), referral to treatment times (including both closed patient pathways and patient pathways waiting to start treatment) and patients who started their first definitive cancer treatment in the month are provided for the month of March 2021.
Data for each topic area is also available in more detail on our StatsWales website and on our interactive dashboard.
Note that data included in this statistical release covers a time period during the coronavirus (COVID-19) pandemic, which has affected both how some NHS services have been offered and people's choices regarding health services. Further information is available in the key quality information section and more detailed commentary on the impact of the pandemic was included in November’s release.
The commentary in this release focusses on changes from the previous month, the same month last year and the same month in the year prior to the pandemic.
Statistician’s comment
This month’s data shows a picture of the NHS now having to manage very high levels of activity in emergency services, in addition to the long term impacts of the COVID-19 pandemic on scheduled care.
More calls were made to the ambulance service than in any month since the pandemic began, with 1 in 13 calls recorded as life threatening (red calls), the highest proportion on record. June was the second busiest month on record for daily attendances to emergency departments and average waiting times in emergency departments increased. Waiting lists for treatments continue to grow with over 600,000 patient pathways waiting to start treatment.
The number of people receiving their first cancer treatments is in-line with pre-pandemic levels and performance against the 62 day target increased slightly in the month. Performance also improved for those waiting for therapy services.
Main points
- There was increased demand on the ambulance service in June 2021, with the highest daily average number of calls recorded since the pandemic began, and the third highest since comparable data was first collected in October 2015.
- In June 2021, a record high percentage of calls to the ambulance service were recorded as immediately life threatening (red calls) since comparable data was first available in May 2019.
- The percentage of red calls receiving a response within 8 minutes was 60.6% in June 2021. This was the same as the previous month, but lower than pre-pandemic levels and below the 65% target for the eleventh consecutive month.
- The number of attendances at emergency departments increased considerably in June 2021 with over 94,000 patients attending, surpassing pre-pandemic levels. The average number of attendances per day was the second highest since comparable data was first collected in April 2012.
- As activity in emergency departments increased in June 2021, performance against both the 4 hour and 12 hour targets decreased, while average waiting times in emergency departments increased to the longest since comparable data was first collected in April 2012.
- The number of patient pathways waiting for diagnostic tests increased in May 2021 compared to April 2021 and the number waiting longer than the target time also increased. While the number of patient pathways waiting for diagnostics has fallen since the height of the pandemic, the waiting list remains markedly higher than before the pandemic started.
- While the number of patient pathways waiting for therapies has increased in every month in 2021, the waiting list remains at a lower level than before the pandemic started. The performance target was not met but performance improved as fewer pathways had waited longer than 14 weeks compared to April 2021.
- The total number of patient pathways who had been referred for treatment but were waiting to start has risen each month since May 2020. In May 2021, there were 608,062 patient pathways waiting to start treatment, the highest since comparable data was first collected in 2011.
- COVID-19 has had a clear effect on performance against both of the referral to treatment targets. Compared with last month, the number of patients waiting longer than 36 weeks increased whilst the percentage of patient pathways waiting less than 26 weeks decreased. The average (median) waiting time for treatment increased slightly when compared to the previous month.
- Experimental statistics show that the number of patients who started their first definitive cancer treatment in the month after being newly suspected of having cancer increased compared with the previous month, and the percentage of patients receiving their first definitive treatment within 62 days of being suspected of having cancer also increased.
Unscheduled care
Emergency calls to the ambulance service
Activity

Emergency ambulance calls and responses to red calls, by local health board and month on StatsWales
Note: An update to call handling practices in May 2019 appears to have resulted in a change to red incident volume. Therefore, it is not possible to compare red incident volumes prior to this time.
The total number of emergency calls received by the Welsh Ambulance Services NHS Trust (WAST) had been increasing gradually over the long term, but call levels fell in most months since the pandemic started. However, the number of calls have been close to or have exceeded pre-pandemic levels since March 2021.
In June 2021, just over 41,000 emergency calls were made to the ambulance service. This is an average of 1,382 calls per day, 45 (3.3%) more calls per day than the previous month, and 237 (20.7%) more calls than the same month last year. This is the third highest average number of calls per day in any month since comparable data was first collected in October 2015.
Calls to the ambulance service are categorised as red, amber or green depending on the urgency of the call. In June 2021, the proportion of all calls that were immediately life-threatening (red calls) was 7.9%, up from 7.4% in May 2021. This is the highest monthly percentage of red calls since comparable red call data was first available in May 2019.
Target
- 65% of red calls (immediately life-threatening – someone is in imminent danger of death, such as a cardiac arrest) to have a response within 8 minutes.

Note: An update to call handling practices in May 2019 appears to have resulted in a change to red incident volume. Therefore it is not possible to fairly compare performance against the target after this date, with performance prior to this date.
Whilst the COVID-19 pandemic is ongoing, emergency response teams have to complete additional procedures including wearing extra personal protective equipment which impacts on the speed at which they can respond to a call.
Performance against the red call target has been mixed over the COVID-19 period. The target was met for each month between April and July 2020; however, performance has since decreased and has generally been lower than the same month before the pandemic started.
In June 2021, 60.6% of emergency responses to immediately life threatening (red) calls arrived within 8 minutes. This is the same as last month but more than ten percentage points lower than in June 2020 and June 2019, and it is the eleventh consecutive month that the 65% target has not been reached.
Analysing average response times provides wider context to performance data. The median waiting time varies from month-to-month, but in the four years prior to the pandemic, has tended to range between 4 minutes 30 seconds and 6 minutes for red calls. However, it has been above 6 minutes for each month since August 2020, reaching a high of 7 minutes 28 seconds in December 2020. In June 2021 the median response time to red calls was 6 minutes 43 seconds. This is 3 seconds faster than in May 2021, but 1 minute and 2 seconds slower than in June 2020.
The majority of calls to the ambulance service are categorised as amber calls. There is no target associated with response times for amber calls but contextual information shows that in June 2021 the median waiting time for amber calls was 60 minutes and 12 seconds. This is more than 12 minutes slower than in May 2021, and more than 37 minutes slower than in June 2020.
Emergency department attendances and admissions to hospital
‘Emergency department’ refers to attendances and admissions at both major accident and emergency departments (A&E), other A&E departments and minor injuries units (MIUs), unless otherwise stated.
A wider range of emergency department performance statistics are now published on the National Collaborative Commissioning Unit (NCCU) website, as management information. This includes measures on the time from patient arrival to triage, the time from patient arrival to contact with a clinical decision maker and analysis of the patient’s discharge destination when they leave the emergency department. These will be updated every month on the same day as this National Statistics publication.
Activity

Note: Chart 3 shows the number of attendances at both major emergency departments and minor injuries units, and the number of admissions resulting from attending major emergency departments only. Admissions from minor injuries units are not recorded on a consistent basis throughout Wales and are therefore not counted in this chart.
While attendances to emergency departments fluctuate each month, attendances are generally higher in the summer months than the winter.
Attendances to all NHS Wales emergency departments have been affected by the COVID-19 pandemic, with sharp falls in attendances in the following spring and winter months, coinciding with waves of the pandemic. Attendances have increased in every month since February 2021, and in June 2021 surpassed pre-pandemic levels with the average number of attendances per day being the second highest on record.
The latest data shows that there were just over 94,000 attendances to all NHS Wales emergency departments in June 2021. This was 7.9% higher than the previous month (6,859 more attendances), 41.8% higher than in the same month last year (27,730 more attendances) and 6.3% higher (5,549 more attendances) than June 2019.
The average number of emergency department attendances per day in June was 3,136. This is 322 more attendances per day on average than in the previous month, 924 more than in the same month in 2020, and 185 more than in June 2019.
The total number of emergency department attendances in the year to June 2021 was 861,723. This is 8.3% lower than the previous year (year ending June 2020) and 19.4% lower than the last 12 month period before the pandemic (March 2019 to Feb 2020).
The trend for admissions to hospital resulting from attendances at major emergency departments, is similar to the trend for attendances to all emergency departments since the pandemic.
In June 2021, 16,272 patients were admitted to the same or a different hospital following attendance at a major emergency department. This is 0.1% lower than the previous month, 12.4% higher than the same month in 2020, but 2.8% lower than the same month in 2019.
Performance
Targets
- 95% of new patients should spend less than 4 hours in emergency departments from arrival until admission, transfer or discharge.
- No patient waiting more than 12 hours in emergency departments from arrival until admission, transfer or discharge.

Performance against 4 hour waiting times target by hospital on StatsWales
Note that this is not a unique count of patients; the same patient will be counted multiple times if they make multiple attendances.
Over the past 5 years, the percentage of patients admitted, transferred or discharged within 4 hours of attending an emergency department has fluctuated from month-to-month but has tended to be close to 80%. During the year prior to the COVID-19 pandemic, the percentage decreased most months, reaching a low point in December 2019, before increasing in early 2020.
During the early months of the pandemic performance against the 4 hour target time improved, reaching a high of 87.1% in May 2020. Since then the trend has been broadly downward and in June 2021, monthly performance was the second lowest since comparable data was first recorded in April 2012.
The latest month’s data shows that 70.6% of patients (66,379 patients) spent less than 4 hours in all emergency care departments from arrival until admission, transfer or discharge. This is 0.5 percentage points lower than the previous month, 14.8 percentage points lower than the same month in 2020, and 7.4 percentage points lower than the same month in 2019. The 95% target continues to be missed.
Contextual information shows that the median time which patients spend in emergency departments has increased gradually from under 2 hours in most months in 2012 and 2013 to around 2 hours and 30 minutes throughout 2019, prior to the COVID-19 pandemic.
During the early part of the pandemic, as attendances decreased the median waiting time decreased, to a low point of 1 hours 48 minutes in April 2020. Since then, median waiting times have increased alongside increasing attendances and reached a record high for the second consecutive month in June 2021.
In June 2021, the median waiting time was 2 hours 49 minutes, up from 2 hours 47 minutes in May 2021 and up from 1 hours 57 minutes in June 2020.
The median time spent in emergency department varies by age. Children generally spend between 1 hour and 30 minutes and 2 hours in emergency department, while older patients (aged 85 or greater) generally spend between 3 hours and 30 minutes and 5 hours in emergency department. However in June 2021, children aged 0-4 waited an average of 2 hours and 29 minutes and adults aged 85 and over waited an average of 5 hours and 50 minutes in emergency departments.

Performance against 12 hour waiting times target by hospital on StatsWales
Note that this is not a unique count of patients; the same patient will be counted multiple times if they make multiple attendances.
The number of patients waiting more than 12 hours to be admitted, transferred or discharged after arriving at an NHS emergency department varies each month but had been on an overall upward trend until the COVID-19 pandemic. Just before the pandemic in January 2020, a little under 7,000 patients waited longer than 12 hours, the highest since current reporting began in April 2012.
In the early months of the COVID-19 pandemic, the number waiting more than 12 hours fell markedly, with April 2020 seeing the lowest number of patients waiting more than 12 hours since current reporting began in April 2012. Since that low point, the number waiting longer than 12 hours has increased and is broadly in-line with levels seen in the months before the COVID-19 pandemic.
In the latest month, 5,950 patients spent 12 hours or more in an emergency care department, from arrival until admission, transfer or discharge. This is an increase of 359 patients (6.4% more) compared to the previous month, an increase of 4,879 (just under six times more) patients compared to the same month in 2020, and an increase of 1,788 (43.0% more) patients compared to the same month in 2019.
Scheduled care activity
Outpatient referrals
Activity

Outpatient referrals on StatsWales
There was a large reduction in the number of referrals for first outpatient appointments in March 2020, during the early weeks of the COVID-19 pandemic. Activity has increased in the months since, but referrals for first appointments remain lower than pre-COVID-19 pandemic level.
An average of 3,312 referrals for first outpatient appointments were made per day in May 2021. This is a decrease of 4.2% (147 fewer referrals per day on average) compared to April 2021. The average number of daily referrals is two times greater than in May 2020 (1,751 more referrals) but there were 13.4% (512) fewer referrals per day on average compared to May 2019.
Diagnostic and therapy waiting times
Activity

Diagnostic and Therapy Services Waiting Times by week on StatsWales
Note: The low point in April 2020 for therapies is in part due to Betsi Cadwaladr not submitting data for this month. To provide likely scale of the impact, data for Betsi Cadwaldr in the two months either side showed that 7,519 were waiting for therapies in March 2020 and 9,840 were waiting in May 2020.
In recent years, prior to the COVID-19 pandemic, the number waiting for diagnostics had been on an upward trend, while the number waiting for therapies had been on a downward trend.
The latest data for May 2021 shows that there were just over 100,000 patient pathways waiting for diagnostics, an increase of 2.7% compared with the previous month. The number of pathways waiting for diagnostics has fallen since its peak in September 2020 but remains 34.4% higher than the same month before the pandemic (May 2019).
The latest data for May 2021 shows that there were just over 41,000 patient pathways waiting for therapies, an increase of 12.1% compared to the previous month. Following the record low in April 2020, the number of patient pathways waiting for therapies was relatively stable for the remaining months of 2020, but has increased in every month in 2021. Despite the recent increases, the latest month’s waiting list is 15.2% smaller than the same month before the pandemic (May 2019).
Performance
Targets
- The maximum wait for access to specified diagnostic tests is 8 weeks.
- The maximum wait for access to specified therapy services is 14 weeks.

Diagnostic and Therapy Services Waiting Times by week on StatsWales
Note: Betsi Cadwaladr did not submit data for April 2020, so are not included in the Wales figures for this month.
Prior to the COVID-19 pandemic starting, there had been a general downward trend in the number of patient pathways waiting 8 weeks or more for diagnostic tests in each month since January 2014 and only a small number of patient pathways waited 14 weeks or more for therapy services.
However, the COVID-19 pandemic has had a clear impact on the number of patient pathways waiting longer than the target times for diagnostic and therapy services. More details are available in the quality information.
The largest number of pathways (62,120) waiting longer than the target time for diagnostics was recorded in May 2020. Since then, the number of pathways waiting longer than the target time has decreased, with some month-to-month fluctuations. At the end of May 2021, just under 42,000 patient pathways waited longer than the target time, an increase of 1.9% compared to the previous month and 11 times greater than the same month before the pandemic (May 2019).
The largest number of pathways (16,056) waiting longer than the target time for therapies was recorded in June 2020. Since then, this number has fallen in most months and at the end of May 2021 there were just under 2,500 patients waiting longer than the target time for therapies. This is a decrease of 15.3% compared to April 2021 but much greater than the 157 patient pathways which were waiting in the same month before the pandemic (May 2019).
Contextual information shows that until the COVID-19 pandemic, median waiting times had been relatively stable for diagnostic tests since 2017 and for therapy services since 2018. Both services saw peaks in median waiting times in June 2020, but median waiting times have generally decreased since then.
In May 2021 the median waiting time for diagnostic tests was 5.6 weeks. This is a decrease from 5.9 weeks in April 2021, a decrease from 11.5 weeks in May 2020 but an increase from 2.7 weeks in May 2019.
In May 2021 the median waiting time for therapy services was 3.6 weeks. This is the same as April 2021, a decrease from 12.4 weeks in May 2020 and a decrease from 3.8 weeks in May 2019.
Referral to treatment time
The referral to treatment time statistics show monthly data on the waiting times for both open and closed pathways following a referral by a GP or other medical practitioner to hospital for treatment in the NHS in Wales. Data for Welsh residents treated or waiting for treatment outside of Wales are not included in the release.
A patient is defined to have been treated, or their pathway closed if either, following consultation with a hospital specialist, no hospital treatment is necessary or if treatment begins. This could include:
- being admitted to hospital for an operation or treatment
- starting treatment that does not require a stay in hospital (for example, medication or physiotherapy)
- beginning the fitting of a medical device such as leg braces
- starting an agreed period of time to monitor the patient’s condition to see if further treatment is needed
COVID-19 has impacted the way treatments are offered. More details are available in the notes section.
Note, the day of referral is defined as the day that the referral letter is received by the hospital.
Activity

The number of patient pathways waiting to start treatment typically varies each month throughout the year, and prior to the COVID-19 pandemic, numbers tended to be highest in late summer and lowest in January.
The COVID-19 pandemic has impacted on the total number of patient pathways waiting to start treatment, with the number increasing steadily every month since May 2020, reaching just over 608,000 by the end of May 2021.This is the highest since comparable data was first collected in 2011.
The number waiting in May 2021 was 2.0% higher (12,048 more patient pathways waiting) than in the previous month, and a third higher than in the May before the pandemic started (May 2019).

Closed patient pathways by month, local health board and weeks waiting on StatsWales
Note Cwm Taf Morgannwg health board have been unable to provide closed pathway data since September 2018. Data for this health board is excluded from the Wales total in the chart to allow for trend analysis.
The number of closed patient pathways varies considerably each month and tends to be lower in April and December, but remained at a broad level close to 80,000 per month for the 3 years prior to the COVID-19 pandemic.
At the start of the pandemic, the number of closed pathways fell sharply with the fewest closed on record in April 2020. In most months since then the number of patient pathways closed has increased, but it has not returned to the pre-COVID-19 level.
The number of patient pathways closed during May 2021 was 60,364, an increase of 1,334 (2.3%) from April 2021, an increase of 32,335 (115.4%) compared with May 2020, but a decrease of 22,054 (26.8%) compared with May 2019.
The average number of patient pathways closed per working day during May 2021 was 3,018, an increase of 67 (2.3%) from April 2021, an increase of 1,543 (over twice as many per day) from May 2020, but a decrease of 906 (23.1%) from May 2019.
Considering changes between comparable twelve month periods reduces the impact of month-to-month variations. There were 620,203 closed pathways during the 12 months to May 2021, a decrease of 28.6% (248,043 fewer pathways) compared to the previous 12 months.
From 16 June 2021 onwards, data relating to Specialist Child and Adolescent Mental Health Services (sCAMHS) has been published alongside other mental health data as StatsWales open data tables.
Performance
Targets
- 95% of patients waiting less than 26 weeks from referral.
- No patients waiting more than 36 weeks for treatment from referral.
During the COVID-19 pandemic, health boards have not performed the same level of validation on referral to treatment performance data as they had previously. Therefore, caution is advised when comparing statistics from March 2020 onwards with previous months. Additional information is provided in the key quality information.
Prior to the COVID-19 pandemic, performance against both referral to treatment targets was fairly stable between 2016 and early 2019, but had been deteriorating since mid-2019.

The percentage of patient pathways waiting less than 26 weeks decreased at the start of the COVID-19 pandemic, reaching the lowest level on record in September 2020. In more recent months there have been some improvements in the percentage of patients waiting less than 26 weeks, but it is still markedly lower than in the pre-pandemic period.
Of the 608,062 patient pathways waiting to start treatment by the end of May 2021, 52.8% (321,066 patient pathways) had been waiting less than 26 weeks. This is a 0.3 percentage point decrease compared to April 2021, a 14.6 percentage point decrease compared to May 2020, and a 34.2 percentage point decrease compared to May 2019.

The number of patient pathways waiting more than 36 weeks has increased since the start of the COVID-19 pandemic, reaching the highest level on record in November 2020. The number remains markedly higher than pre-pandemic figures.
In May 2021, 227,753 patient pathways (37.5% of all patient pathways waiting to start treatment) had been waiting more than 36 weeks from the date the referral letter was received by the hospital. This is an increase of 5,369 (2.4%) compared to April 2021, more than three times as many compared to May 2020 and eighteen times as many compared to May 2019.
Contextual information shows that the median waiting time to start treatment had generally been around 10 weeks between late 2013 and February 2020, but this has increased since the pandemic started. The median waiting time was 23.6 weeks in May 2021 this is a slight increase from 23.4 weeks in April 2021, an increase from 18.2 weeks in May 2020 and an increase from 9.5 weeks in May 2019.
Cancer services
Cancer services have remained open throughout the pandemic but have needed to operate at reduced capacity. Data relating to cancer services during the initial period of the COVID-19 (coronavirus) pandemic is available in statistical releases published prior to February 2021.
This publication now solely includes data from the suspected cancer pathway data collection. This is to align with the introduction of a suspected cancer pathway target, which was introduced on the 18 November 2020, and effective for all patients treated on the suspected cancer pathway from 1 December 2020. More information on these changes can be found in the February 2021 statistical release.
The ‘number of people entering the single cancer pathway’ will continue to be published on StatsWales. These data are still collected directly from health boards, using aggregate data collection forms, and not via the new centralised data collection using the National Data Resource through Digital Health and Care Wales.
More details on this change are available in the quality information.
Suspected cancer pathway (experimental statistics)
The suspected cancer pathway starts at the point of suspicion (for example when a GP makes a referral) and this is when the recorded waiting time starts. The pathway is closed, and the waiting time ends, if the patient: starts their first definitive treatment;
- is told they do not have cancer (downgraded)
- chooses not to have treatment
- if the patient dies
The data does not include suspensions and for this reason the data is only comparable with the historical single cancer pathway data collection for the number and percentage of patients starting treatment within 62 days without suspensions.
This publication focusses on data relating to three headline statistics on the suspected cancer pathway, these are:
- number of patients informed they do not have cancer
- number of patients treated who started their first definitive treatment
- number and percentage of patients who started their first definitive treatment within the 62 day target time (without suspensions)
A number of wider measures from the suspected cancer pathway produced by Digital Health and Care Wales have been published alongside this statistical release, to provide more context to the activity and performance of cancer services in Wales. More information on the suspected cancer pathway is available in the key quality information.
Activity

Suspected cancer pathway (closed pathways) on StatsWales
In May 2021, 10,320 patients were informed they do not have cancer. This is a decrease of 3.4% (363 patients) compared to April 2021.
In May 2021, 1,529 patients newly diagnosed with cancer started their first definitive treatment in the month. This is an increase of 5.0% (73 patients) from April 2021 and an increase of 65.3% (604 patients) from May 2020.
Performance
Target
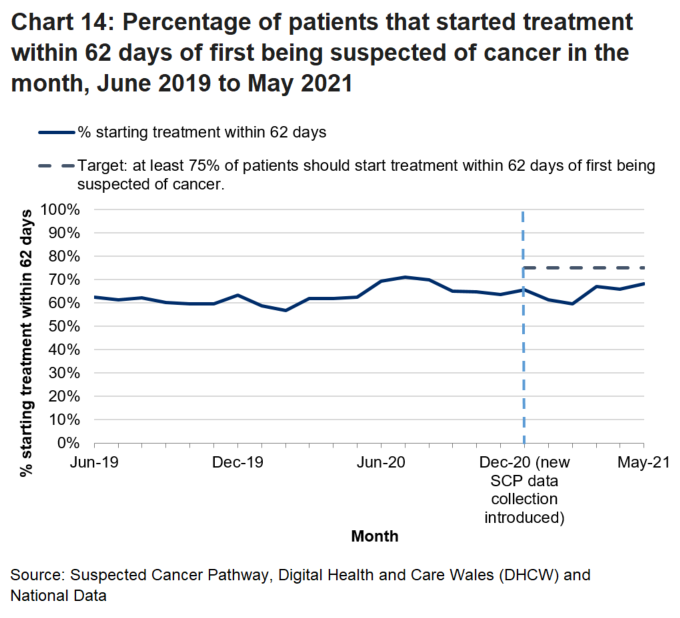
- At least 75% of patients should start treatment within 62 days (without suspensions) of first being suspected of cancer. This target will be reviewed at a later date. Data published for time periods before December 2020 are not subject to the target.
Suspected cancer pathway (closed pathways) on StatsWales
In May 2021, 68.2% of patients (1,043 out of 1,529) newly diagnosed with cancer started their first definitive treatment in the month within 62 days of first being suspected of cancer. This is 2.3 percentage points higher than in April 2021 and 5.6 percentage points higher than May 2020.
Quality information
Changes to NHS Wales Informatics Service (NWIS)
On 1 April 2021 the function of NHS Wales Informatics Service was replaced with a new organisation called Digital Health and Care Wales. It has been created to take forward digital transformation and provides the national technology and data services needed by patients and clinicians. They operate as a Special Health Authority with an independent Chair and Board. There has been no impact on the data supplied to the Welsh Government for this statistical release.
Data quality during the COVID-19 pandemic
During the COVID-19 pandemic resources across all NHS organisations have been stretched, including those responsible for recording, processing and validating data. This means that some of the data included in this statistical release may not have been subject to the same rigorous validation checks that would normally have occurred prior to the pandemic. While data submitted during the pandemic is of broadly good quality, there are some data specific data quality issues.
- Betsi Cadwaladr health board did not submit data for the number of pathways waiting for therapy services in April 2020. This affects diagnostic and therapy services activity and performance data in that month only.
- Neath Port Talbot hospital was unable to submit blood pressure monitoring, echo cardiogram and heart rhythm sub-specialty data for August and September 2020.
- Princess of Wales hospital was unable to submit consultant, gastroscopy and MRI sub-specialty data for August and September 2020. This affects diagnostic and therapy services activity and performance data in Cwm Taf Morgannwg, Swansea Bay and at a Wales level in those months.
- While referral to treatment waiting lists remain active, clinicians have had to review all patients on the waiting lists at various stages to identify clinical priorities. The amount of validation performed by local health boards on waiting list data has been reduced as the same resources are also focused on supporting the new ways of working. This affects the referral to treatment activity and performance data.
- While not COVID-19 specific, Cwm Taf Morgannwg has not submitted closed pathways data since September 2018 (Cwm Taf health board between September 2018 and March 2019). Therefore closed pathways data only refers to the six other health boards to allow for trend analysis at a national level.
Ambulance response times
During the COVID-19 pandemic emergency response staff have been required to wear additional personal protective equipment which will impact how quickly they can respond to a call. In addition, after an ambulance has been dispatched to the scene, it must then go through additional cleaning processes to prevent the spread of the virus. This results in the vehicle being taken off the road for a time which may also affect response times during this period.
As part of the continual review of the clinical response model, the Welsh Ambulance Service Trust regularly reviews call handling practices and the categorisation of incidents. An update to call handling practices in May 2019 appears to have resulted in a change to red incident volume. Therefore, it is not possible to compare red incident volumes prior to this time. Increases in red incident volumes may also impact on performance due to the additional resources required to attend a red incident.
The clinical response model for ambulance services was introduced in Wales from 1 October 2015. The trial, initially scheduled for 12 months, was extended for a further 6 months, but, following receipt of the independent evaluation report commissioned by the Emergency Ambulance Services Committee (EASC), the clinical response model was implemented (February 2017). See the quality report for more details.
There are three overarching call categories.
- Red: Immediately life-threatening (someone is in imminent danger of death, such as a cardiac arrest).
- Amber: Serious, but not immediately life-threatening (patients who will often need treatment to be delivered on the scene, and may then need to be taken to hospital).
- Green: Non urgent (can often be managed by other health services and clinical telephone assessment).
The categorisation of a call is determined by the information given by the caller in response to a set of scripted questions, which is then triaged by the automated Medical Priority Dispatch system (MPDS). Call handlers are allowed up to two minutes to accurately identify both the severity and nature of a patient’s condition (for those calls that are not immediately life threatening). An ambulance or other appropriate resource is dispatched as soon as the severity and condition are identified. In high acuity calls, this may be whilst the caller is still on the line. There are two occasions where the priority of a call could be changed; when new information from the caller is assessed via the MPDS system, or where a nurse or paramedic has gathered further information about the patient’s condition over the phone.
For the purposes of the 8 minute target, the clock starts when the patient’s location and chief complaint has been established.
Revisions: Any revisions to the data are noted in the ‘Notes for this month’s publication’ and in the information accompanying the StatsWales cubes each month.
Ambulance services: StatsWales
Ambulance services: Quality report
Ambulance services: Annual release
Emergency departments
The term ‘emergency department’ captures activity at major accident and emergency (A&E) departments, other A&E departments and minor injury units (MIUs).
Note that the number of admissions to hospital are based on attendances at only major emergency departments in Wales. This is because admissions to hospital from attendances at minor injuries units are not recorded consistently across Wales.
On 17 November 2020, a new major emergency department opened at the new Grange University hospital in the Aneurin Bevan health board. The Grange University Hospital contains a host of specialist services in one place, including a 24 hour emergency department and assessment unit for major emergencies and resuscitations which could require onward intensive care.
In data referring to December 2020 onwards, both Royal Gwent and Nevill Hall hospitals have been re-classified to “Other emergency department/Minor Injury Units - Other emergency department/Minor Injury Units” following the opening of the Grange University hospital. This category of hospital is defined as all other emergency department/casualty/minor injury units which have designated accommodation for the reception of accident and emergency patients and can be routinely accessed without appointment, but which do not meet the criteria for a major emergency department. This also means that statistics for admissions from major emergency departments will not include admissions from attendances at Royal Gwent or Nevill Hall hospitals from December 2020s data onwards.
Major emergency departments are defined as a consultant led service with resuscitation facilities and accommodation for the reception of emergency department patients. Major emergency departments must provide the resuscitation, assessment and treatment of acute illness and injury in patients of all ages, and services must be available continuously 24 hours a day.
During the COVID-19 pandemic, several minor injury units (MIUs) temporarily closed, but some have since reopened. These are Barry hospital (closed in March 2020; reopened in September 2020); Bryn Beryl Hospital (closed in May 2020; reopened in September 2020); Dolgellau and Barmouth District Hospital (closed in April 2020; remains closed); Tywyn & District War Memorial Hospital (closed in June 2020; remains closed); and Llandovery Community Hospital (closed in April 2020; remains closed).
Since 5 August 2020 the CAV24/7 service has been in operation in Cardiff and Vale University Health Board, which affects how services are delivered in its emergency departments. The ‘Phone First’ model encourages patients who think they have an urgent need to attend an emergency department but do not have an immediately life threatening condition to call ahead to be pre-triaged. Depending on the severity of the condition, they may be encouraged to self-care; signposted to a more appropriate service in their local community; or directly booked in to a timeslot in an emergency department if they need further assessment and treatment.
Other health boards are working towards introducing similar services but none are yet in operation.
In terms of measuring the time a patient spends waiting, the clock start time remains unchanged: the time starts when the patient physically arrives at the emergency department. While the service is in its infancy extra validations will be performed on Cardiff and Vale’s data to assess the impact of the changes. To date, neither the level of activity or performance against the two emergency department targets has changed markedly since the service was introduced.
Alongside these National Statistics three new measures have been developed as part of the Emergency Department Quality Delivery Framework (EDQDF). This framework developed a broader range of measures, to provide more context about delivery of care in emergency departments. These include measures on the time from patient arrival to triage, the time from patient arrival to contact with a clinical decision maker, and analysis of the patient’s discharge destination when they leave the emergency department.
As the datasets and data collection processes for these measures are developed, they are published as management information on the National Collaborative Commissioning Unit (NCCU) website on the same day as this publication. Dependent on data being robust and meeting the requirements of the Code of Practice for Statistics, Welsh Government intend to publish these alongside our official statistics in 2021, with an experimental statistics status in the first instance.
From March 2021, amendments have been made to the NCCU’s data extraction methodology, meaning their figures for the number of attendances to major emergency departments will match those published in this National Statistics publication. Figures published by NCCU for previous months have also been revised based on their new methodology.
Digital Health and Care Wales provide the data from the Emergency Department Data Set (EDDS). This is a rich source of patient level data on attendances at emergency care facilities in Wales that tends mainly to be used for the performance targets.
Targets: Time spent in emergency departments.
- 95% of new patients should spend less than 4 hours in emergency departments from arrival until admission, transfer or discharge.
- No patient waiting more than 12 hours in emergency departments from arrival until admission, transfer or discharge.
Revisions: Some figures are likely to be revised in future months. Each submission from health boards contains data for up to the last 12 months. This may contain minor revisions to previously published periods. The revised data will be published on StatsWales with the latest month. Any substantial revisions will be footnoted and mentioned in the stats release.
Comparability and coherence: Figures produced for Wales, Scotland and Northern Ireland are National Statistics. All four UK countries publish information on the time spent in emergency departments/Accident and Emergency (A&E), though this can be labelled under Emergency Department (as in Scotland) or Emergency Care (as in Northern Ireland). The published statistics are not exactly comparable because: they were designed to monitor targets which have developed separately within each country; the provision and classification of unscheduled care services varies across the UK; the systems which collect the data are different.
Time spent in emergency departments: StatsWales
Time spent in emergency departments: Quality report
Time spent in emergency departments: Annual release
Outpatient referrals
Revisions: From December 2015, the revisions policy is to revise back every 12 months on a monthly basis.
Aneurin Bevan health board had previously not provided data for the adult mental illness treatment speciality for March and April 2021, but this has now been provided and data has been revised.
Comparability and coherence: Similar information is available from other parts of the UK but the data is not exactly comparable due to local definitions and standards in each area. Data standards and definitions have been agreed across health boards ensuring that data is collected on a consistent basis across Wales.
Outpatient referrals: StatsWales
Outpatient referrals: Quality report
Diagnostic and Therapy waiting times (DATS)
The increased number of pathways waiting for diagnostics is directly linked to the impact of COVID-19 with all non-urgent outpatient appointments suspended in March 2020 in order to prioritise urgent treatments. In addition, while more services have since restarted, additional infection, prevention and control measures have been implemented that has affected the amount of diagnostic testing activity that can be carried out.
Conversely, the lower level of patient pathways waiting for therapies during the height of the pandemic is in part due to carrying out many of these services virtually. As a result, a higher volume of patients received an appointment than if they were all conducted in-person at a hospital setting.
Note that Betsi Cadwaladr health board did not submit therapies data for April 2020. This affects the number of total patient pathways waiting in the month and data for this month should not be compared with other months, at the Wales level. To give an estimate of the scale of the impact, there were 25,501 pathways waiting in the other six health boards in April 2020, while in the two months either side, there were 7,519 patient pathways waiting in March 2020 and 9,840 in May 2020, in Betsi Cadwaladr.
This will also affect the number and percentage of pathways waiting longer than the target time. Performance data for April 2020 is only representative of the six health boards which provided data for that month. No data has been estimated for the missing data in this release or on StatsWales.
Targets: Waiting times for access to diagnostic and therapy services (operational standards for maximum waiting times).
- The maximum wait for access to specified diagnostic tests is 8 weeks.
- The maximum wait for access to specified therapy services is 14 weeks.
Revisions: Any revisions to the data are noted in the ‘Notes for this month’s publication’ and in the information accompanying the StatsWales cubes each month.
Comparability and coherence: See notes for Referral to Treatment.
Diagnostic and Therapy waiting times: StatsWales
Diagnostic and Therapy waiting times: Quality report
Diagnostic and Therapy waiting times: Annual release
Referral to treatment times
A referral to treatment pathway (RTT) covers the time waited from referral to hospital for treatment and includes time spent waiting for any hospital appointments, tests, scans or other procedures that may be needed before being treated. Definitions of terms used and quality information are in the quality report.
Targets: Referral to treatment times:
- 95% of patients waiting less than 26 weeks from referral to treatment.
- No patients waiting more than 36 weeks for treatment.
Cwm Taf Morgannwg (and Cwm Taf prior to April 2019) have been unable to provide closed pathway data since September 2018 because of IT problems following a software update. Therefore, all numbers and comparisons for closed pathways from the October 2018 release onwards exclude Cwm Taf Morgannwg. The data for Cwm Taf for previous months are available on StatsWales.
At the end of June 2019, Cwm Taf Morgannwg advised the Welsh Government that they thought there was an issue with the reporting of certain RTT waiting lists. They asked the NHS Wales Delivery Unit to carry out a review and this resulted in a total of 1,783 additional patients being added to the RTT waiting list for the publication of July 2019 data in October 2019. In addition, the Delivery Unit also carried out a review of the diagnostic waiting list and found an additional 1,288 patients should have been reported. These patients were also added to the official figures for the end of July 2019 that were reported in October 2019. Whilst the patients were not reported as part of the official statistics they were being reported internally to the health board. Welsh Government has contacted other health boards and has been advised that all waiting lists are being reported as per the Referral to Treatment Guidelines.
Treatments conducted virtually are counted the same as in-person activity, and since the COVID-19 pandemic, a higher volume of treatments have been conducted virtually.
As all non-urgent outpatient appointments were suspended in March in order to prioritise urgent appointments, the length of waiting times for patients referred for treatment has increased markedly. In addition, while more services have since restarted, additional infection, prevention and control measures have been implemented that has affected the amount of treatment activity that can be carried out.
At present, clinicians are reviewing all the patients on the waiting lists at various stages to identify clinical priorities. While referral to treatment waiting lists remain active, the amount of validation performed by local health boards on waiting list data has been reduced as resources are also focused on supporting the new ways of working. Caution should be taken when comparing performance statistics from March 2020 onwards with previous months due to these changes.
Data previously collected via the long-standing PP01W data collection for treatment specialties not included in RTT ceased following an impact assessment, therefore statistics based on this collected have also ceased.
Revisions: Any revisions to the data are noted in the ‘Notes for this month’s publication’ and in the information accompanying the StatsWales cubes each month.
Comparability and coherence: England, Scotland and Wales publish referral to treatment waiting times that measures the complete patient pathway from initial referral e.g. by a GP, to agreed treatment or discharge, in addition to certain stages of treatment waiting times. Northern Ireland publish waiting times statistics for the inpatient, outpatient and diagnostics stages of treatment that measures waiting times for the different stages of the patient pathway, typically specific waits for outpatient, diagnostic or inpatient treatment, or for specific services such as audiology.
To increase consistency across health board data, all new treatment codes have been amended to their pre-April 2016 equivalents. This has now been actioned for all historic RTT and referrals data. This will be implemented until all health boards are able to report using the new codes consistently. For more information, see this Data Set Change Notice (2014/08).
In relation to referral to treatment waiting times, whilst there are similar concepts in England, Wales and Scotland in terms of measuring waiting times from the receipt of referral by the hospital to the start of treatment, and, the types of patient pathways included, there are distinct differences in the individual rules around measuring waiting times. This is particularly important regarding ‘when the clock stops or pauses’, exemptions, and the specialities covered.
Referral to treatment: StatsWales
Referral to treatment: Quality report
Referral to treatment: Annual release
Cancer Services
Cancer patients are treated by clinical urgency rather than length of wait. COVID-19 has affected how cancer services are delivered. Health boards have needed to adapt through various means including implementing additional infection, prevention and control measures to ensure they are delivering safe services while reducing the risk of patients contracting COVID-19. This has meant services have been operating at reduced capacity.
The number of patients starting treatment within the target time will also likely to be affected by the periods where some patients were shielding and by patient choices.
Suspected cancer pathway
From February 2021, data is only published for the suspected cancer pathway. For more information on the pathway, see this Data Set Change Notice with these key documents.
The suspected provides a more transparent and meaningful method for measuring performance of cancer services, compared to the previous urgent and non-urgent pathways. It does this by measuring the time on the cancer pathway from the point a patient was suspected of having cancer rather than the point at which the decision to treat is made. All patients are included regardless of their routes of referral who have started their first definitive treatment in the reporting period. This includes patients who were referred to secondary care in Wales but may receive treatment outside of NHS Wales (in both a different country and private hospitals), but does not include patients with a recurrence of the original primary cancer.
This data collection is based on closed pathway data and measures activity through the number of patients being treated or being informed by a specialist that they do not have cancer, rather than the number of patients entering the pathway.
The suspected cancer pathway target is: At least 75% of patients should start their first definitive treatment within 62 days (without suspensions) of first being suspected of cancer. This target was effective from 1 December 2020.
Targets for the urgent and not via the urgent pathway have ceased and no new data will be collected or published for these pathways. Historical data remains available on the StatsWales website.
The number of people entering the pathway (i.e. those suspected of having cancer) is still being collected directly from health boards using an aggregated data collection form. This will continue until development work has been completed and a new method of collecting this data is finalised. Data for the number of patients entering the pathway has experimental statistics status as it may contain some duplicate referrals or may not contain data from all referral sources. For these reasons, the data will provide a broad idea of scale and trend but is limited in its use and more detailed inferences would be of low reliability.
Alongside the move to solely reporting on the suspected cancer pathway, a range of wider contextual performance measures have been developed. An analysis of these measures has been brought together using the National Data Resource at Digital Health and Care Wales and has been published by Welsh Government as an Digital Health and Care Wales product. This dashboard is in continuous development and will aim to contain analysis of: the median time to first appointment, the median time for patients to be informed of a positive diagnosis for cancer, and the median number of days to a patient’s first diagnostic test when data are of sufficient quality. Breakdowns by age group and sex are also presented. This data is also published with experimental statistics status.
Revisions: Any revisions to the data are noted in the ‘Notes for this month’s publication’ and in the information accompanying the StatsWales datasets each month.
Comparability and coherence: Other UK countries also measure cancer waiting times. However, the outputs differ in different countries because they are designed to help monitor policies that have been developed separately by each government. Further investigation would be needed to establish whether the definitional differences have a significant impact on the comparability of the data.
A detailed analysis of historical cancer waiting times is also published in an annual statistical release.
Historically, data for Powys for those patients who entered the pathway only showed patients who were later downgraded as not having cancer, and this continues with the suspected cancer pathway collection.
Specialist Child and Adolescent Mental Health Services (sCAMHS)
From 16 June 2021 onwards, data relating to Specialist Child and Adolescent Mental Health Services (sCAMHS) has been published alongside other mental health data as StatsWales open data tables.
Delayed transfers of care (DToC)
At the start of the COVID-19 pandemic, the Welsh Government suspended delayed transfers of care reporting requirements, along with many other datasets. In the interim, Welsh Government introduced the COVID-19 Discharge Requirements, which included a new discharge process with increased focus on rehabilitation and reablement.
The Welsh Government and the NHS Delivery Unit have been collecting interim weekly delayed discharge data to provide management information to support the new arrangements. This data does not measure delayed transfers of care in the same way as the previous data collection, and has not been assessed against the standards of the Code of Practice for Statistics. Options for future collection and publication of data and performance measures will be developed as soon as possible, as work in this area has been delayed due to other priorities relating to COVID-19 pandemic.
Sources
Ambulance response data is provided by the Welsh Ambulance Service NHS Trust (WAST).
All other data summarised here is collected from local health boards by the Digital Health and Care Wales. Full details are provided in the Quality reports for each service area.
Timeliness
Publishing our monthly NHS activity and performance releases on the same day provides users with a more rounded and integrated picture of activity and gives a more coherent view of the NHS in Wales.
Not all datasets have the same processing timelines. To make the data available as soon as we can, we publish the unscheduled care data for, say, October alongside the planned care data for September.
Data
Online tool, an interactive online tool has been developed with three sections.
- Demand and activity, for example, emergency departments attendances, ambulance calls, referrals.
- Performance, for example, performance against emergency departments targets, RTT etc.
- Context, for example, median time in emergency departments, median ambulance response times, median RTT waits
All charts show the latest five year period, if data has been collected on a comparable basis for that long. Note the exception to this are the ambulance activity and performance charts, where an update to call handling practices in May 2019 appears to have resulted in a change to red incident volume. Therefore, it is not possible to compare red incident volumes prior to this time.
Further detailed datasets can be found, downloaded or accessed through our open data API from StatsWales.
Percentage point changes are calculated using unrounded figures.
Contextual information
Charts presented in the online tool provide additional activity information to complement the NHS performance information shown above.
Some charts include median and mean times. For example, in relation to ambulance response times.
- The median response time is the middle time when all emergency responses are ordered from fastest to slowest, so half of all emergency responses arrive within this time. It is commonly used in preference to the mean, as it is less susceptible to extreme values than the mean.
- The mean response time is the total time taken for all emergency responses divided by the number of emergency responses. The mean is more likely to be affected by those ambulances which take longer to arrive at the scene.
Revisions
Information relating to revisions is presented in the ‘Notes for this month’s publication’ and in the information accompanying the StatsWales datasets each month.
Relevance
What are the potential uses of these statistics?
These statistics will be used in a variety of ways. Some examples of these are:
- advice to ministers
- to assess, manage and monitor NHS Wales performance against targets
- to inform service improvement projects for areas of focus and opportunities for quality improvement
- by NHS local health boards, to benchmark themselves against other local health boards
- to contribute to news articles on waiting times
- to help determine the service the public may receive from NHS Wales
Who are the key potential users of this data?
These statistics will be useful both within and outside the Welsh Government. Some of the key potential users are:
- ministers and their advisors
- members of the Welsh Parliament and the Members Research Service in the Welsh Parliament
- local health boards
- local authorities
- The department for Health and Social Services in the Welsh Government and other areas of the Welsh Government
- National Health Service Wales
- Public Health Wales
- the research community
- students, academics and universities
- individual citizens and private companies
- media
The statistics may also be useful for other UK governments
Northern Ireland Executive’s Department of Health, Social Services and Public Safety
Scottish Government
Department of Health in England
Comparability
All four UK countries publish information on a range of NHS performance and activity statistics. The published statistics are not exactly comparable because: they were designed to monitor targets which have developed separately within each country; the provision and classification of unscheduled care services varies across the UK. Statisticians in all four home nations have collaborated as part of the ‘UK Comparative Waiting Times Group’. The aim of the group was to look across published health statistics, in particular waiting times, and compile a comparison of (i) what is measured in each country, (ii) how the statistics are similar and (iii) where they have key differences. That information is available on the Government Statistical Service website. Information on ambulances can be found at:
Ambulance services in Scotland
Ambulance services in Northern Ireland
National Statistics status
Aside from single cancer pathway statistics, the Office for Statistics Regulation has designated all other statistics presented in this release as National Statistics, in accordance with the Statistics and Registration Service Act 2007 and signifying compliance with the Code of Practice for Statistics.
National Statistics status means that our statistics meet the highest standards of trustworthiness, quality and public value, and it is our responsibility to maintain compliance with these standards.
All official statistics should comply with all aspects of the Code of Practice for Statistics. They are awarded National Statistics status following an assessment by the UK Statistics Authority’s regulatory arm. The Authority considers whether the statistics meet the highest standards of Code compliance, including the value they add to public decisions and debate.
It is Welsh Government’s responsibility to maintain compliance with the standards expected of National Statistics. If we become concerned about whether these statistics are still meeting the appropriate standards, we will discuss any concerns with the Authority promptly. National Statistics status can be removed at any point when the highest standards are not maintained, and reinstated when standards are restored.
NHS Wales Cancer Waiting Times, Ambulance Services in Wales, Time Spent in NHS Wales Accident and Emergency Departments, NHS Referral to Treatment Times, NHS Wales Diagnostic & Therapy Services Waiting Times and Delayed Transfers of Care in Wales are National Statistics.
The continued designation of these statistics as National Statistics was confirmed in 2011 following a compliance check by the Office for Statistics Regulation. These statistics last underwent a full assessment against the Code of Practice in 2011.
Experimental Statistics
Statistics relating to the suspected cancer pathway are Experimental Statistics. This is to inform users of the data and its reported statistics are still in a developmental phase and may have issues pertaining to data quality. However, the statistics are still of value provided that users view them in the context of the data quality information provided. As the dataset matures the coverage and the quality of the data being reported will improve enabling the data to become fit for a wider variety of beneficial uses.
These are official statistics which are published in order to involve users and stakeholders in their development and as a means to build in quality at an early stage.
All official statistics should comply with all aspects of the Code of Practice for Official Statistics. They are awarded National Statistics status following an assessment by the UK Statistics Authority’s regulatory arm. The Authority considers whether the statistics meet the highest standards of Code compliance, including the value they add to public decisions and debate.
More information on the use of experimental statistics.
Well-being of Future Generations Act (WFG)
The Well-being of Future Generations Act 2015 is about improving the social, economic, environmental and cultural well-being of Wales. The Act puts in place seven well-being goals for Wales. These are for a more equal, prosperous, resilient, healthier and globally responsible Wales, with cohesive communities and a vibrant culture and thriving Welsh language. Under section (10)(1) of the Act, the Welsh Ministers must (a) publish indicators (“national indicators”) that must be applied for the purpose of measuring progress towards the achievement of the Well-being goals, and (b) lay a copy of the national indicators before Senedd Cymru. The 46 national indicators were laid in March 2016.
Information on the indicators, along with narratives for each of the wellbeing goals and associated technical information is available in the Wellbeing of Wales report.
Further information on the Well-being of Future Generations (Wales) Act 2015.
The statistics included in this release could also provide supporting narrative to the national indicators and be used by public services boards in relation to their local wellbeing assessments and local wellbeing plans.
Next update
19 August 2021
We want your feedback
We welcome any feedback on any aspect of these statistics which can be provided by email to stats.healthinfo@gov.wales.
Contact details
Statistician: Rhys Strafford
Telephone: 0300 025 0058
Email: stats.healthinfo@gov.wales
Media: 0300 025 8099
SFR 218/2021