Technical Advisory Group: advice for 5 August restriction review
Advice from the Technical Advisory Group and the Chief Scientific Advisor for Health for 5 August restriction review.
In this page
This report provides advice on the proposed relaxations considered as part of the 5 August 2021 review, covering:
- Face coverings
- TTP and Self-isolation rules
- Nightclub mitigations
- Any use of a ‘COVID pass’
TAC advice is sought to inform this review, ensuring the revised basket of indicators to reflect the emergence of the delta variant set out in the updated Coronavirus Control Plan published on 14 July are encompassed.
This advice is informed by a range of evidence sources, including from the Scientific Advisory Group for Emergencies (SAGE), the Welsh Government Technical Advisory Group (TAG) and subgroups, Public Health Wales, the Wales COVID-19 Evidence Centre, and the wider academic literature and surveillance data.
Advice from previous review cycles is referred to where relevant and is not repeated here.
Summary
Overall, the most recent modelled scenarios from Swansea University suggest that it is likely cases, hospitalisations and deaths will remain flat or increase slightly during July, and then begin to increase again in August as restrictions are eased further (on 7 August).
Cases peaked in mid July 2021 and are estimated to peak again around September 2021. Hospitalisations and deaths are estimated to peak a couple of weeks after cases but at a lower level than previous waves.
In this third wave, we are still in a race between vaccines and the Delta variant, with school closures acting as a potential firebreak but increased mixing from easing restrictions acting as an additional opposing force.
Vaccines are having to do more heavy lifting in a high prevalence world – vaccines might be less effective as force of infection increases.
Even when high uptake of vaccination is successful in reducing the harm arising from severe clinical outcomes in infected individuals, high levels of community transmission remain associated with significant risks, not least the emergence of new variants of concern.
When schools return there will likely be continued high transmission in children and young people so a measured policy response needs to be developed to this.
Although there has been a recent signal of declining case numbers, the wastewater signal suggests the infection cases have not declined in several areas.
Evidence on the effectiveness of face covering to reduce the spread of transmission of SARS-CoV-2 in the community and efficacy of different types of face coverings remains limited and conclusions rely on low quality sources of evidence with high risk of bias. Evidence suggests that face coverings may provide benefits in preventing transmission of SARS-CoV-2 but higher quality studies suggest these benefits may be modest.
Recent TAG advice on nightclubs and adult entertainment venues remains extant. This advice concluded that nightclubs represent a higher risk of transmission. It is unclear at present what impact a fully vaccinated population would have upon the risk and probability level of infection.
Revision of the TTP system such that isolation of double vaccinated individuals is relaxed is likely to lead to a small increase in the reproduction number (Rt), with a slightly bigger increase if the policy also applies to under 18s, who are largely unvaccinated. Modelling does not consider any potential impacts of periodic PCR testing of vaccinated contacts or the likelihood of vaccinated contacts becoming infected.
Wales situation update
Previous TAG 21-day review advice is still extant and this paper seeks to build on that advice. The most recent situational assessment for Wales is documented in the COVID-19 Situational Report and the most recent TAC brief.
Cases across Wales have increased rapidly since the beginning of June, following a six-month sustained reduction in cases. The cases appear to be mainly in younger people, notably those aged 10-29, which suggests that vaccination is providing a degree of protection, but there is some evidence of spread to older groups.
Comparison of current levels with previous waves continues to support that the link between cases, deaths and hospitalisations has been weakened by the vaccination programme, although it has not been broken entirely and these have all increased alongside cases, although to a lesser extent than previous waves.
Over the last few days there is indication of plateauing rates, possibly starting to decline. It is too early to know if the latter is just a short-lived response to the end of the school term, or a more meaningful improvement. We are awaiting unbiased estimates of infection from ONS Covid Infection Survey which is lagged by around a week. It is also not known whether the reduction reflects a similar reduction in test seeking behaviour for younger adult. Fewer tests have been undertaken over the past week. Case positivity rates are high at 10.8% at a national level for the 7 day period ending 23 July.
Figure 1. Case and testing rates per 100,000 in each UK Nation
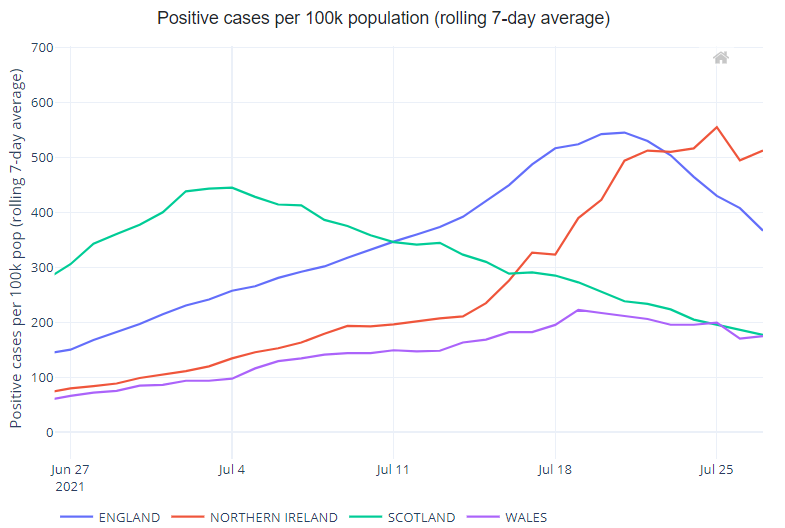
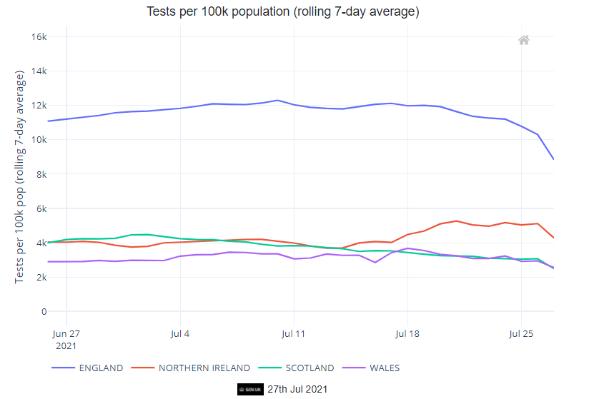
We might reasonably expect hospitalisations and ICU admissions to continue to increase for the coming weeks.
At present cases are tracking close to the most likely scenario, as are hospital admissions, however critical care admissions and occupancy are tracking closer to the reasonable worst case, although still much lower than previous waves in absolute terms. This discrepancy could reflect altered thresholds for clinical decision making about critical care need. Deaths continue to be very low; slightly lower than the most likely scenario. The most likely scenario predicts a sustained level of cases between now and around November time, but there is uncertainty over this.
If the population continue to practise sensible protective behaviours e.g. social distancing, reducing contacts, seeking vaccination, isolating on symptoms etc. and baseline measures are continued then changes to level zero are less likely to result in unmanageable levels of cases; however a return to high epidemic levels is not impossible. We are in uncharted territory with high cases in a highly vaccinated population, staying close the data, surveillance and local intelligence will be key. Reverse engineering relaxations swiftly might be required if conditions deteriorate.
Data from the ONS Covid-19 Infection Survey states that in Wales, the percentage of people testing positive continued to increase in the week ending 24 July 2021; ONS estimate that 18,800 people in Wales had COVID-19 (95% credible interval: 12,700 to 26,000), equating to around 1 in 160 people. It is important that this lagged but unbiased indicator of community prevalence continues to be monitored closely.
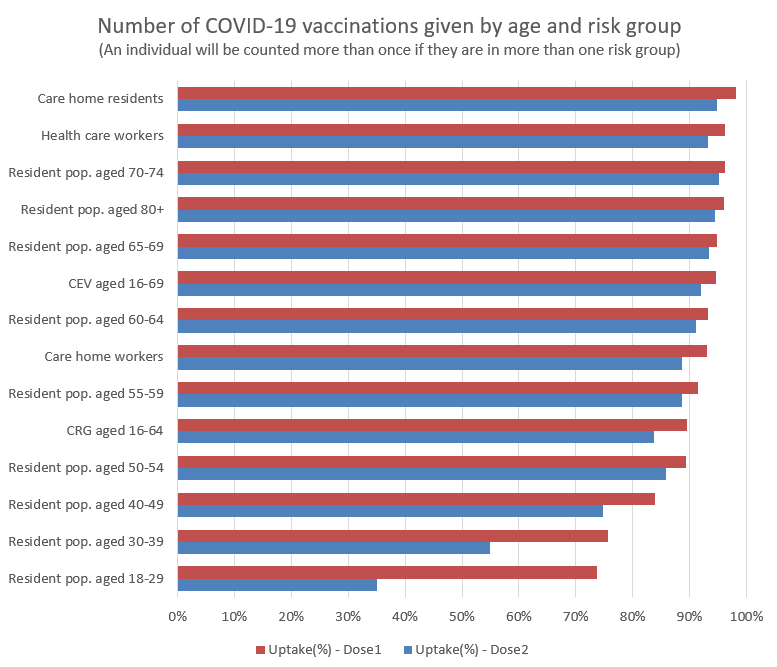
As of 14 June, all adults in Wales have been offered a vaccine. Vaccine rollout is continuing, although the number of weekly first dose vaccinations has decreased significantly and second dose numbers have begun to slow since June (Figure 2). This leaves first dose uptake in the 18-29 and 30-39 age groups at around 75% as the focus moves to second dose vaccination (Figure 3).
Figure 2. Vaccination population coverage in Wales (1 and 2 doses)
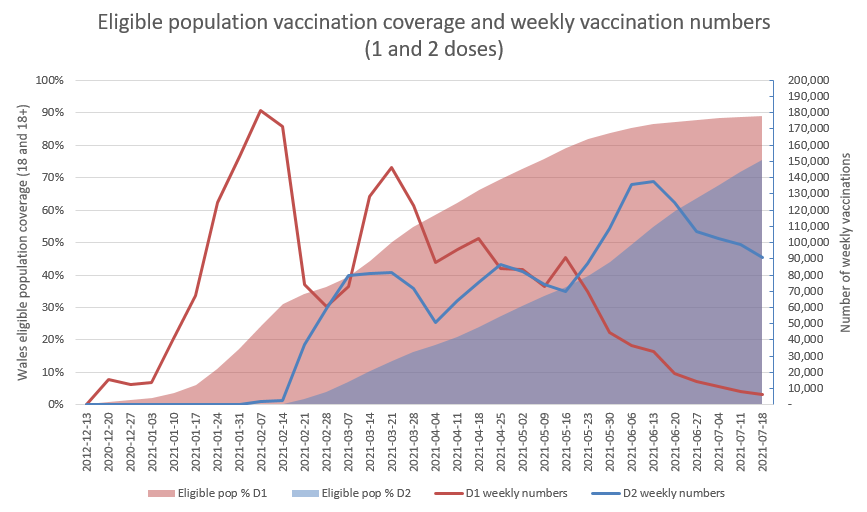
Figure 3. Vaccination coverage in Wales by group and age
As reported by Welsh Government, the number of adult care homes which have notified Care Inspectorate Wales of one or more confirmed cases of COVID-19, in staff or residents, in the last 7 and 20 days generally decreased from January 2021, however, there has been a steady increase since 2 June 2021 (Figure 4).
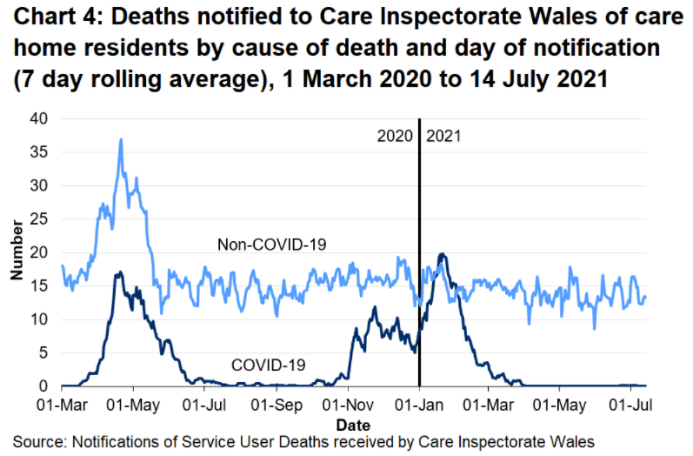
Between 27 March 2021 and 21 June 2021, there were no reported deaths of care home residents relating to suspected or confirmed COVID-19. There were two reported care home resident deaths between 22 and 30 June 2021 but there have been no reported deaths since then (Figure 5).
Figure 4: number of adult care homes who have notified CIW of one or more confirmed cases of COVID-19 in the past 7 or 20 days, up to 14 July
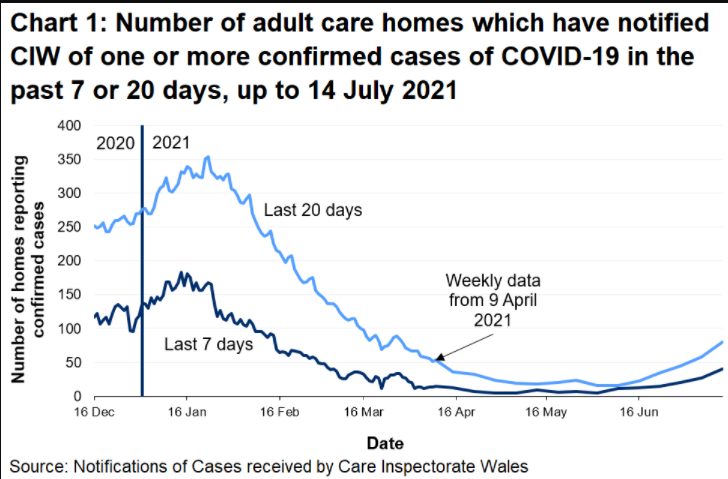
Figure 5: deaths notified to CIW of care home residents by cause of death and day of notification (7 day rolling average up to 14 July)
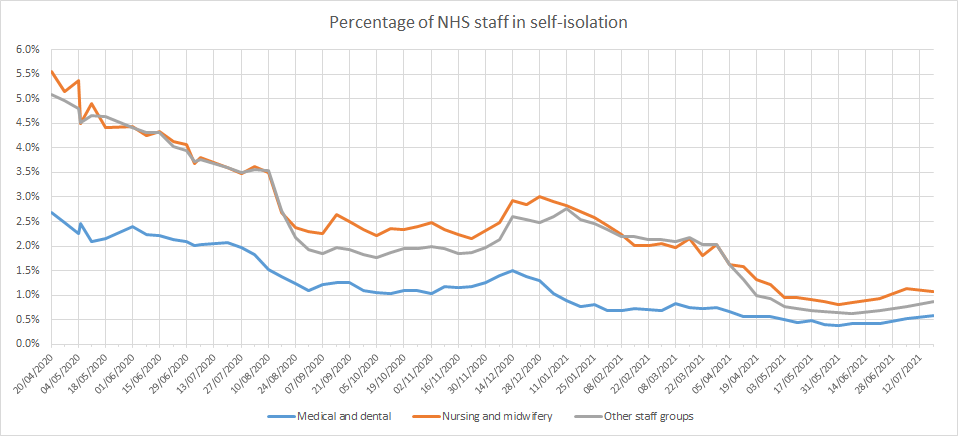
The percentage of NHS staff self-isolating decreased through April 2020 to May 2021 but has increased slightly since the beginning of June to between 0.6% for medical and dental staff to 1.1% for nursing and midwifery staff (figure 6).
Figure 6: percentage of NHS staff in self-isolation split by profession
Source: StatsWales
Wastewater monitoring
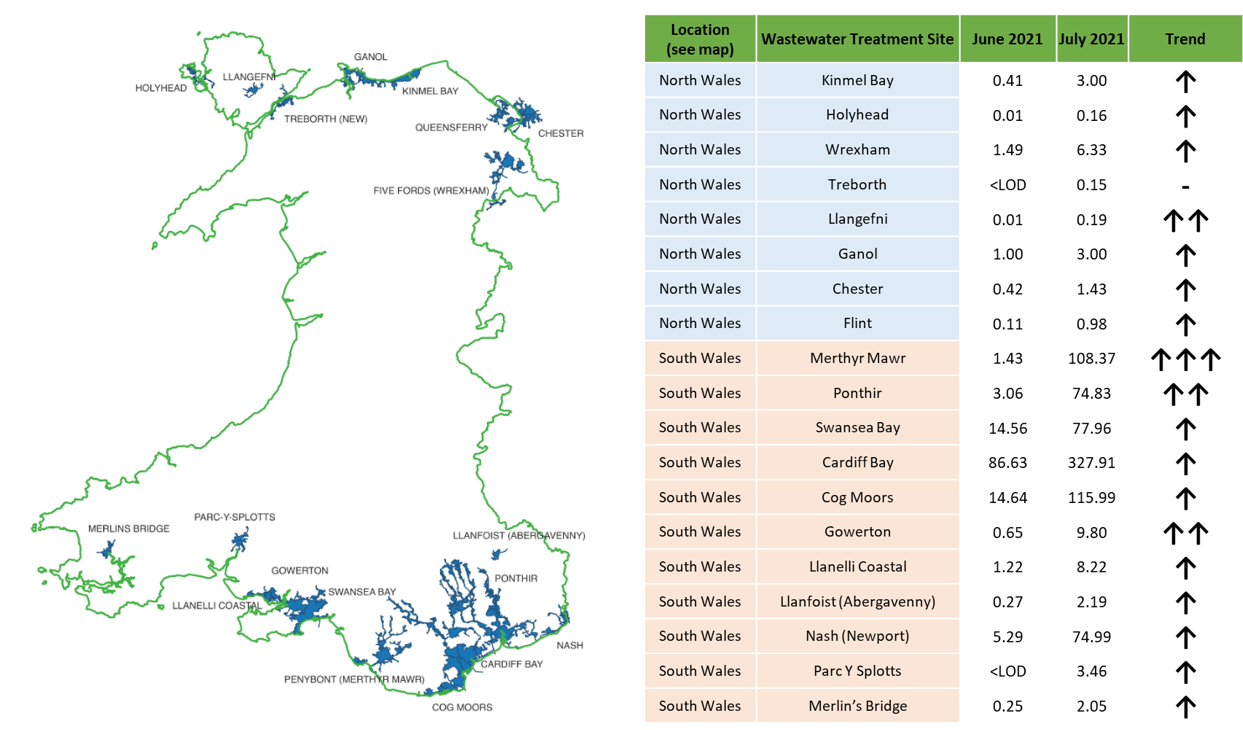
The monitoring of wastewater for SARS-CoV-2 offers an indicator unbiased by testing policy and behaviour changes. In Wales, samples obtained from 20 wastewater treatment works (WwTWs) 3-5 times a week. This approach covers approximately 70% of the population.
The analysis of wastewater is complex, with levels measured in samples only being reliable intelligence when adjusted, or ‘normalised’ for the flow rates into WwTWs. Flow is not directly measures at sites, but reliable proxies have been developed over some time and are utilised in the Welsh, Scottish and JBC wastewater programmes.
The collection and analysis of wastewater is undertaken by the Waste Water Monitoring Project, managed by TAC and delivered by the consortium of Bangor University, Cardiff University and Dŵr Cymru.
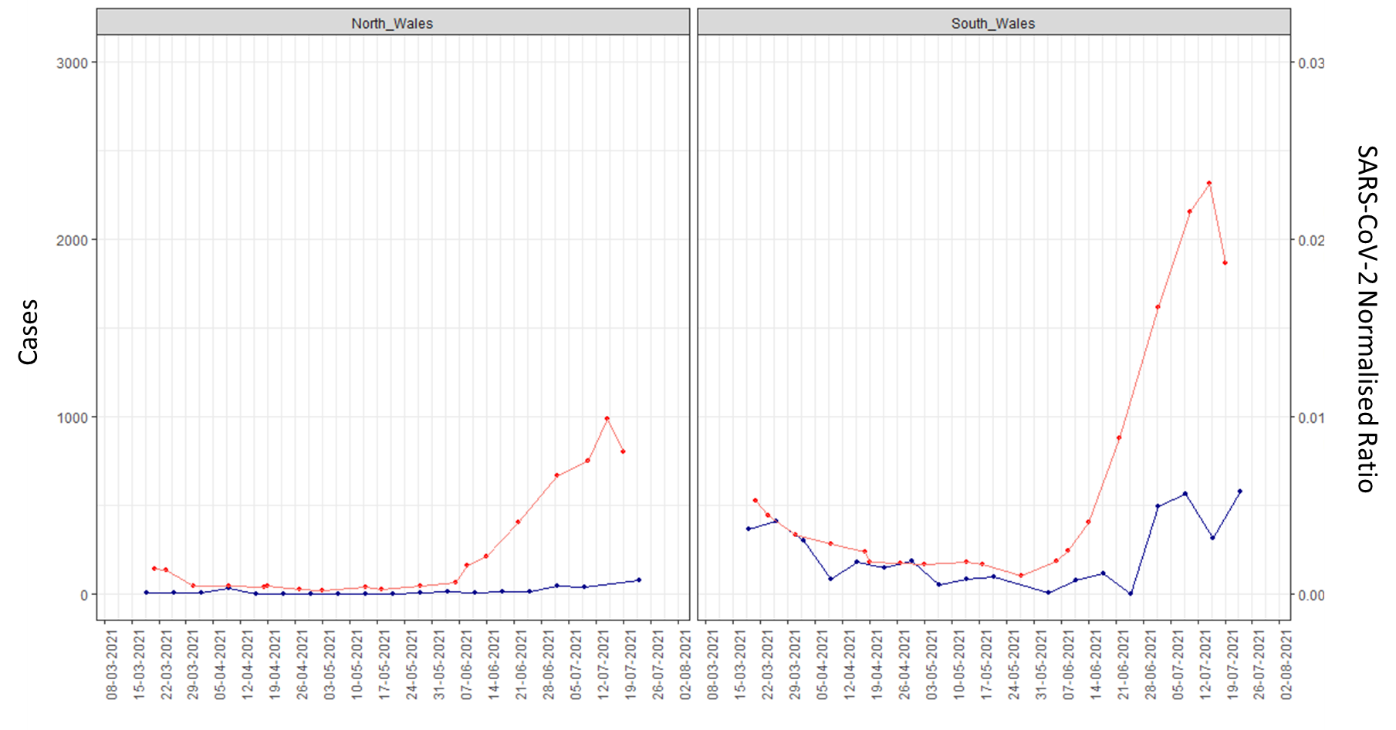
Generally, the wastewater SARS-CoV-2 signal up to the 19 July 2021 at a national level was confirmatory of the national trend in positive test cases up to the same period.
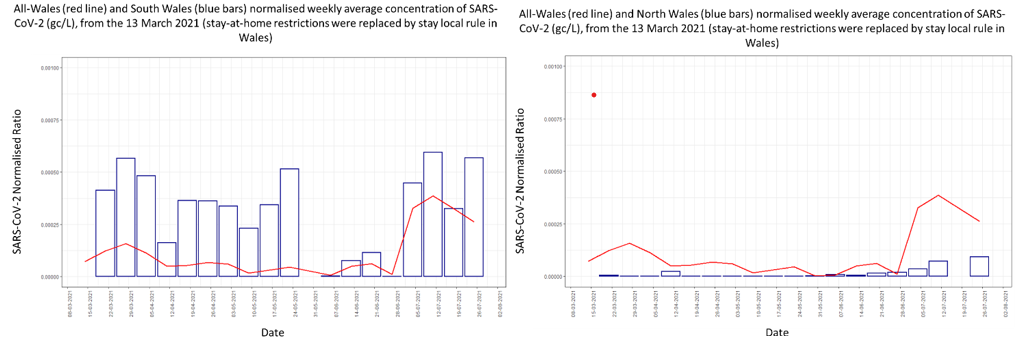
However, at some sites in North and South Wales, there have been substantial increases in the wastewater levels of SARS-CoV-2 (normalised and unnormalised) over the past 4-6 weeks.
North and South Wales weekly new COVID-19 case data within the wastewater catchments (red) and normalised concentration of SARS-CoV-2 (gc/L) from wastewater (blue), from the 13 March 2021 (stay-at-home restrictions were replaced by stay local rule in Wales)
Case numbers by LSOA, source: PHW
In South Wales up to the w/e 25 July 2021 the Swansea, Bridgend and Abergavenny sites continue to show increasing levels of SARS-CoV-2 detected in wastewater despite the number of cases detected though community testing having declined in that same period. Despite the case numbers declining the wastewater signal suggests the infection cases have not declined in those areas.
In North Wales up to the w/e 25 July 2021 the Wrexham, Anglesey (Llangefni) and Kinmel Bay sites continue to show increasing levels of SARS-CoV-2 detected in wastewater despite the number of cases detected though community testing having declined or remained stable in that same period. Despite the case numbers declining the wastewater signal suggests the infection cases have not declined in those areas.
Despite these localised trends, the other monitored sites show a decrease in the presence of SARS-CoV-2 in wastewater by the w/e 25 July 2021.
Changes in average mean normalised concentration of SARS-CoV-2 (gc/L) at each of the wastewater treatment sites, scaled for population size. (LOD, limit of detection) Number of arrows indicates relative magnitude of the increase
Reasonable Worst Case (RWC) scenarios versus actual figures
Observed levels of COVID-19 cases, admissions to hospital, deaths and hospital bed occupancy are roughly at the levels estimated by the June 2021 MLS scenarios. COVID-19 admissions to ICU and ICU occupancy are following the reasonable worst case (RWC) scenario more closely, but are still relatively low in absolute terms.
All COVID-19 indicators increased throughout July, but cases and admissions to ICU are showing signs of decreasing. There is a risk as the season for RSV has started around 15 weeks earlier than usual, which may lead to critical care bed demand in very young children as well as some older adults. If influenza season also starts early, this may lead to usual NHS winter pressures occurring in Summer.
Updated modelling
A modelling update is available in the most recent TAC brief (annex 1). Two opening scenarios are also included- one in which contacts return to pre-pandemic levels on 7 August (rapid return) and another in which ongoing protective behaviours delay this return until 1 December (gradual). The results highlight the importance of encouraging a baseline level of population protective behaviours at this stage in the pandemic, despite the excellent progress of the vaccination programme.
Cases are currently tracking with the lower estimates of ‘delta-mid’ or the upper-end of ‘delta low’. Current modelling suggests that cases could soon begin to plateau, partly as a result of reduced contact networks during the school break, although if all baseline population protective behaviours were to end following the 7 August announcement modelling (rapid return scenario) estimates a subsequent increase in cases, deaths and hospitalisation.
Note that even once all non-pharmaceutical interventions are lifted it is likely that some level of population-level behaviours will remain for a period, so the ‘rapid return’ scenario should be interpreted as a hypothetical worst case rather than a realistic scenario, although there is considerable uncertainty around population behaviours in the longer term and the impact of factors such as waning immunity and the risk of novel variants of concern.
Face coverings
- There are several potential baseline measures available which can reduce transmission of COVID-19 once we move to level 0. The most effective, with high adherence, continues to be those that reduce the likelihood that people who are infectious mix with others in the population, such as isolation [footnote 1]. This is followed by reducing the likelihood of those potentially infectious people who are not isolated entering high risk settings or situations, such as certification or ‘COVID-passes’. Finally there is decreasing the transmission risk from an infectious person in any environment, using environmental or administrative controls such as improving ventilation [footnote 2] and wearing of face coverings.
- The evidence around face coverings and face masks have previously been considered in several papers published by TAG and SAGE [footnote 3]. As previously advised, face coverings can be effective in reducing transmission in public and community settings (medium confidence) [footnote 4]. Their effectiveness stems mostly from reducing the emission of virus-carrying particles when worn by an infected person (source control). They may provide a small amount of protection to an uninfected wearer; however, this is not their primary intended purpose (medium confidence). Widespread application of face coverings as a source control is likely to have a small but significant impact on population level transmission, though the benefit is difficult to quantify.
- Contamination of face coverings is likely to increase with duration of wearing and therefore the risk of transmission via touching or surface contamination from more heavily contaminated face coverings could increase with time (low confidence). It is therefore recommended that use of face coverings is considered in situations where they may be required for longer periods, though tolerability and equity need to be considered [footnote 5]. Consideration should continue to be given to disadvantaged groups who could be adversely affected (e.g. hard of hearing, young children in education settings).
- A recent rapid evidence review undertaken by the Wales COVID-19 Evidence Centre [footnote 6] considered the following questions:
- What is the effectiveness of face coverings to reduce the spread of transmission of SARS-CoV-2 in the community (i.e. non-healthcare settings)?
- What is the efficacy of different types of face coverings designed for use in community settings?
Key findings
- Evidence on the effectiveness of face covering to reduce the spread of transmission of SARS-CoV-2 in the community and efficacy of different types of face coverings remains limited and conclusions rely on low quality sources of evidence with high risk of bias. The quality of observational studies could be improved by methods that better address confounding factors.
- Evidence suggests that face coverings may provide benefits in preventing transmission of SARS-CoV-2 but higher quality studies suggest these benefits may be modest.
- There was no evidence about the effectiveness of face coverings to prevent transmission of SARS-CoV-2 in specific community settings (e.g. specifically in educational settings or public transport); specifically for children & adolescents; in different seasonal conditions; the extent of protection for wearers or others. Where evidence is available, it is from comprehensive application across settings.
- Evidence suggests that commonly used face coverings have some efficacy in filtering droplets. Medical masks appear to have a higher efficacy than fabric masks although some studies suggested equivalent efficacy.
- Studies recorded harms sub-optimally but there was no indication of serious harms from wearing face coverings. Some people report discomfort or the feeling of breathing difficulty (rates varied substantially – 15% to 75% – across 3 studies). There are also environmental concerns about the extent of non-biodegradable products.
- Face coverings are usually part of a bundle of measures (hand hygiene, distancing, ventilation etc.) and most evidence is in this context. Mask-wearing alone, in the absence of other preventive measures, may not be effective.
- There may be benefits from providing public health messages on characteristics of face coverings that appear to have higher efficacy (i.e. medical masks) and effective use of masks (covering nose and mouth).
The full report will be published shortly.
PHE Human challenge studies
- Emerging data from Human Challenge Studies where young, healthy, volunteers were exposed to SARS- CoV-2 in a safe and controlled environment will continue to be considered. The findings are awaiting publication in a journal and will be shared once the paper is published.
- These initial studies will help to increase understanding about how the immune system reacts to coronavirus and identify factors that influence how the virus is transmitted, including how a person who is infected with COVID-19 virus transmits infectious virus particles into the environment.
[1] EMG, SPI-M and SPI-B: Considerations in implementing long-term ‘baseline’ NPIs, 22 April 2021 (GOV.UK)
[2] Royal Academy of Engineers- Infection Resilient Environments, 16 July 2021
EMG: Role of ventilation in controlling SARS-CoV-2 transmission, 30 September 2020 (GOV.UK)
EMG: Simple summary of ventilation actions to mitigate the risk of COVID-19, 1 October 2020 (GOV.UK)
[3] Technical Advisory Group: use of face coverings in childcare and educational settings for Under 18s - 19 June 2021
Technical Advisory Cell: use of face coverings in the context of COVID-19 - 9 June 2020
Technical Advisory Group: updated advice on face coverings - 14 August 2020
SPI-B: Sustaining behaviours to reduce SARS-CoV-2 transmission, 30 April 2021
NERVTAG/EMG: Duration of wearing of face coverings, 15 September 2020
Potential impact of face covering on the transmissibility of SARS-CoV-2 in the UK, 20 April 2020
[4] EMG: Application of physical distancing and fabric face coverings in mitigating the B117 variant SARS-CoV-2 virus in public, workplace and community, 13 January 2021 (GOV.UK)
[5] Fifty-seventh SAGE meeting on COVID-19 (publishing.service.gov.uk)
[6] Rapid review of face coverings to reduce transmission of SARS-CoV-2. Report RR00007. Wales COVID-19 Evidence Centre. July 2021 (In press, available on request).
Nightclub mitigations
Recent TAG advice on nightclubs and adult entertainment venues remains extant. This advice concluded that nightclubs represent a higher risk of transmission. International evidence also suggests potential issues with providing proof of a negative COVID test prior to entry, which may have resulted in a super-spreading event.
It is unclear at present what impact a fully vaccinated population would have upon the risk and probability level of infection. The biggest threat to this is higher prevalence levels and the introduction of new Variants of Concern which may have the ability to escape immunity.
Use of ‘Covid Pass’
- Much of the evidence to date refers to what have been termed immunity passports or certificates, which provides proof the holder is fully vaccinated, has had a prior COVID-19 infection or a recent negative test result. Such a certificate was required, for example, to gain entry to recent events forming part of the Events Research Programme in England.
- More recently, emphasis has been placed on a narrower vaccine passport, providing evidence the holder is fully vaccinated. For example, this form of passport has been identified by the UK Government as being required for entry to nightclubs in September and most recently, to Premier League football matches, by which point the vast majority of adults would have been offered both doses of a COVID-19 vaccine.
- SAGE has previously considered broader immunity certification in a number of papers [footnote 7].
- Immunity certification should not permit the relaxation or avoidance of self-isolation if symptoms develop. Certificates should also not be used to replace other measures to protect high-risk individuals. Certification could be used in addition to other measures used to control transmission and/or to enable the relaxation of certain measures, but it is an imperfect tool and a risk-based approach should be adopted. The prevalence of infection in the community will have an important impact on the level of risk and effectiveness of certification (it may be very effective when prevalence is low, but less effective at high prevalence). The reliability of any immunity certificate will be reduced if virus variants with significant antigen escape are circulating. [footnote 8]
- Due to the limited evidence around the outcomes if certification is to be introduced, SAGE has previously recommended use of pilot studies to understand the impact and practicalities of certification, including consideration of behavioural and ethical issues [footnote 9]. Communication to the public on any certification policy will be important, with regards to what a test means in practice, particularly on individual safety and potential effect on others. Attitudes towards certificates can also vary between different groups. Certificates also should not imply that an individual has no risk, rather they have a reduced risk.
- A recently published review [footnote 10] by a number of academics attending SPI-B (based on earlier work by SPI-B [footnote 11]) looked at immunity passports. While the evidence is very limited, the authors suggest there is a public health case for the introduction of immunity certificates to enable greater and safer access to international travel, events such as sports, music and theatre, while also facilitating a return to pubs, restaurants and cafes. Certification requiring vaccination could also encourage vaccine uptake. However, several concerns have also been identified, notably the possibility of perverse incentives (e.g. deliberate infection), complacency with regard to other personal protective behaviours (e.g. social distancing or use of face coverings) and the possibility of increased opposition to vaccination among some groups. The review also highlights concerns raised in relation to ethical and legal issues, including privacy, discrimination, crime and loss of social cohesion.
- In terms of crime and legitimacy, the SPI-B Policing and Security sub-group [footnote 12] (December 2020) suggested certification would likely be more acceptable if seen as enabling rather than restricting, allowed early release from isolation or access to services. Potential demand on GPs was raised if people contacted them for proof (a point also made here [footnote 13]), while enforcement could also add to the burden on public–facing staff. The potential for crime is noted and while steps could be taken to minimise this with digital technologies, reassurance would be needed for those less comfortable using mobile apps and requiring a paper version (e.g. the digitally excluded).
- With specific reference to vaccine passports, a Moral and Ethical Advisory Group (MEAG) paper to SAGE [footnote 14] (December 2020) also notes the potential social and economic benefits associated with such a passport. The strongest ethical case for this approach arises where vaccination gives the holder immunity from becoming infected, while also preventing them from transmitting the disease. However, as is pointed out, there is no guarantee COVID-19 could not be contracted or passed on and clear communication would be critical given the potential false sense of security a passport could provide. The briefing concludes ‘It would be reasonable to suggest that a high degree of confidence would be required that those vaccinated would not be asymptomatic carriers before certification was adopted’.
- More recently [footnote 15] (April 2021), in considering issues of access, equity and ethics associated with vaccine passports, the potential for incentivising vaccine uptake has been reinforced, with national and international benefits. The continued restriction of civil liberties for those who pose minimal risk of transmission could be seen as unethical, although the long-term effectiveness of available vaccines would need to be continuously monitored, particularly with possibility of new variants emerging. Similar concerns to those noted above are also identified, including the potential for coercion and stigmatisation [footnote 16], difficulties for certain groups with vaccine access problems (e.g. pregnant women) or those known to be hesitant (e.g. minority ethnic groups). Practical issues around internet access, privacy and data protection would also need to considered.
Looking specifically at the potential impact of vaccine passports on inclination to get vaccinated, a recent preprint [footnote 17] (June 2021) presents UK data from a large scale survey and modelling exercise carried out in April 2021. The findings suggest the introduction of vaccine passports will likely lower the inclination to get vaccinated once baseline vaccine intent has been adjusted for, the decrease being larger if passports were used for domestic purposes (i.e. not for international travel). The authors conclude passports may result in lower vaccine inclination in socio-demographic groups that cluster geographically, possibly contributing to concentrated areas of low uptake and an epidemic risk.
[7] NERVTAG: Immunity certification, 9 December 2020
Academics: Ethics of certification – briefing paper, 9 December 2020
NERVTAG: Certifying COVID-19 immunity, 19 November 2020
[8] NERVTAG: Immunity certification update, 4 February 2021 (GOV.UK)
[9] SPI-B: Health status certification in relation to COVID-19, behavioural and social considerations, 9 December 2020 (GOV.UK)
[10] Behavioural responses to COVID-19 health certification: a rapid review | BMC Public Health | Full Text (biomedcentral.com)
[11] SPI-B: Health status certification in relation to COVID-19, behavioural and social considerations, 9 December 2020 (GOV.UK)
[12] SPI-B Policing and Security Subgroup: Health status certification in relation to COVID-19 legitimacy and enforcement considerations, 9 December 2020 (GOV.UK)
[13] COVID-19: Certifying status for “vaccine passports” must not increase GPs’ workload, says Royal College (The BMJ)
[14] Academics: Ethics of certification – briefing paper, 9 December 2020 (GOV.UK)
[15] COVID-19 vaccine passports: access, equity, and ethics (The BMJ)
[16] COVID-19 antibody testing and ‘immunity certification’ - The Nuffield Council on Bioethics (nuffieldbioethics.org)
[17] The potential impact of vaccine passports on inclination to accept COVID-19 vaccinations in the United Kingdom: evidence from a large cross-sectional survey and modelling study (medRxiv)
TTP and self-isolation of contacts
The updated Coronavirus control plan for Wales was published in July 2021. It set out what Alert level zero would look like for Wales when it enters it on 7 August 2021. Vaccinations have helped to weaken the link between confirmed COVID-19 cases and hospitalisations and/or deaths. However, an increase in COVID-19 cases still remains a concern and efforts should still be taken to reduce chains of transmission. Test, Trace, Protect will need to adapt to respond to the pandemic over the coming months to remain proportionate to the risks from COVID-19 and the wider harms.
The intention is to remove the requirement for people who are fully vaccinated to self-isolate if they are a close contact of someone who has tested positive. Discussions with stakeholders are ongoing regarding the requirements for children and young people who are contacts to self-isolate. Final decisions will be made as part of the next review, due by 5 August 2021. In the meantime the existing rules apply. However, those with symptoms of coronavirus or those testing positive will need to self-isolate whether fully vaccinated or not.
This paper considers the impact of the self-isolating rules changing as stated above. We consider what would happen if we stop self-isolation for contacts in the following scenarios:
- Either all contacts
- Or all under 18s and all fully vaccinated
This report updates previous modelling of the TTP system published in March 2021.[footnote 18] This report focuses on the potential impact of changing the requirements for contacts to self-isolate.
Data from the Welsh TTP system on the observed delays and efficiency of each component was used to estimate the percentage of transmissions that may have occurred from an index case or their contacts before they were traced and entered isolation. This was then used to estimate an approximate effect on the reproduction number, R.
Given the observed R value in Wales, the characteristics of TTP at the time can be used to try and infer the value of R in the absence of TTP. During winter high transmission and prevalence (outside of firebreak), we estimated TTP reduced R from approximately 1.7 to 1.3. Using R values in February 2021 and improvements to case ascertainment and test and trace times, the effect may have been a reduction from approximately 1.3 to 0.8.
Using a recent R value (SPI-M, 15 July 2021), TTP may have reduced R from around 2.2 to 1.4. If TTP were to continue but with the requirement of fully vaccinated contacts and under 18s to self-isolate removed, then R is estimated to increase from 1.4 to approximately 1.7. Removing both of these requirements therefore is estimated to increase R by around 0.3. We note the magnitude of the impact changes with the absolute R value, and hence changes over the dynamics of the epidemic. At a value of R around 1, the estimated increase is 0.2.
| Contacts Traced | Reff realised | Estimated R in absence of TTP (counterfactual) | Impact of TTP on R | Additional R compared to Full |
|---|---|---|---|---|
| Full (trace 90%) | 1.4 (as observed) | 2.22 | 0.82 | - |
| No u18s (trace 63%) | 1.55 | 2.22 | 0.67 | 0.15 |
| No vaccinated (trace 72%) | 1.51 | 2.22 | 0.71 | 0.11 |
| No u18s or vaccinated (trace 45%) | 1.66 | 2.22 | 0.56 | 0.26 |
In the absence of TTP, R is estimated to be 2.22 when ascertainment of infections are assumed to be 40%. A full TTP response is estimated to reduce R to 1.4, an absolute reduction of 0.82. Removing the requirement of contacts aged under 18 or fully vaccinated contacts to isolate reduces R from 2.22 to 1.55 and 1.51 respectively. Removing both of these requirements is estimated to reduce R from 2.22 to 1.66. Therefore, removing both of these requirement will lead to an R value 0.26 higher than the current full TTP.
Vaccine effectiveness analysis by Public Health England supports that vaccines are effective in reducing the likelihood of severe outcomes and preventing symptomatic infection; isolation of contacts is currently causing wider impacts on infrastructure and individuals and models show a limited impact on Rt if vaccinated contacts don’t isolate. Vaccines may also reduce the likelihood of a person becoming infected, and the Public Health England Vaccine Surveillance Report estimates vaccinated individuals in a household study in England had a 35-50% reduced risk of becoming infected, although estimates of effectiveness against transmission are primarily from a period when Alpha was the dominant COVID-19 variant. This is following a single dose and the effect on transmission is likely to be greater with two doses.
| Vaccine status | Vaccine effectiveness | |
|---|---|---|
| Alpha | Delta | |
| Dose 1 | 49 (46 to 52) | 35 (32 to 38) |
| Dose 2 | 89 (87 to 90) | 79 (78 to 80) |
Source: PHE
| Vaccine status | Vaccine effectiveness | |
|---|---|---|
| Alpha | Delta | |
| Dose 1 | 78 (64 to 87) | 80 (69 to 88) |
| Dose 2 | 93 (80 to 97) | 96 (91 to 98) |
Source: PHE
[18] Technical Advisory Group: modelling the current Welsh Test, Trace, Protect system (GOV.WALES) published on 24 March